English
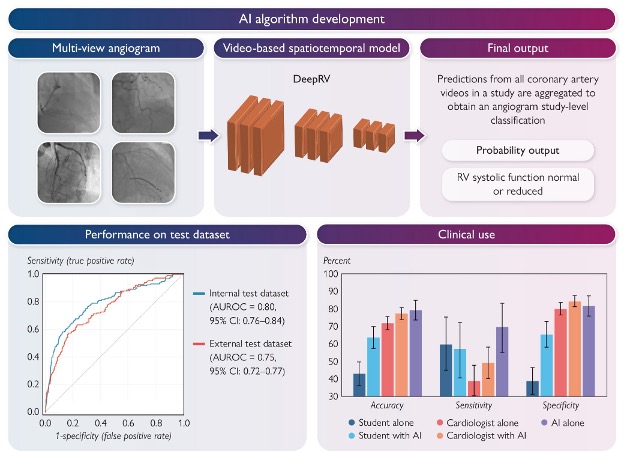
Right ventricular systolic function (RVSF) is a critical determinant of cardiovascular outcomes — yet rapid bedside RVSF assessment during coronary angiography is often impossible when prior echocardiography is unavailable, especially in acute coronary syndromes. We developed and validated DeepRV, an open-weight video-based deep neural network that predicts reduced RVSF directly from routine coronary angiograms.
Transthoracic echocardiography is the gold standard for RVSF, but acoustic windows are often poor in critically ill patients and TTE is rarely immediately available in the cath lab. Coronary angiograms are already acquired in nearly every ACS patient — they encode systolic motion of the epicardial vessels, which carries information about underlying cardiac mechanics. DeepRV extracts an RV-specific signal from these routine videos.
DeepRV was trained on 8,053 angiographic studies from 6,035 patients at the Montreal Heart Institute (2017–2023), with RVSF labelled by paired transthoracic echocardiography per 2025 ASE guidelines (TAPSE, fractional area change, visual assessment). It was externally validated on 2,247 studies from UCSF (27.7% reduced RVSF prevalence) and prospectively deployed at MHI on 82 consecutive STEMI cases via the PACS-AI platform.
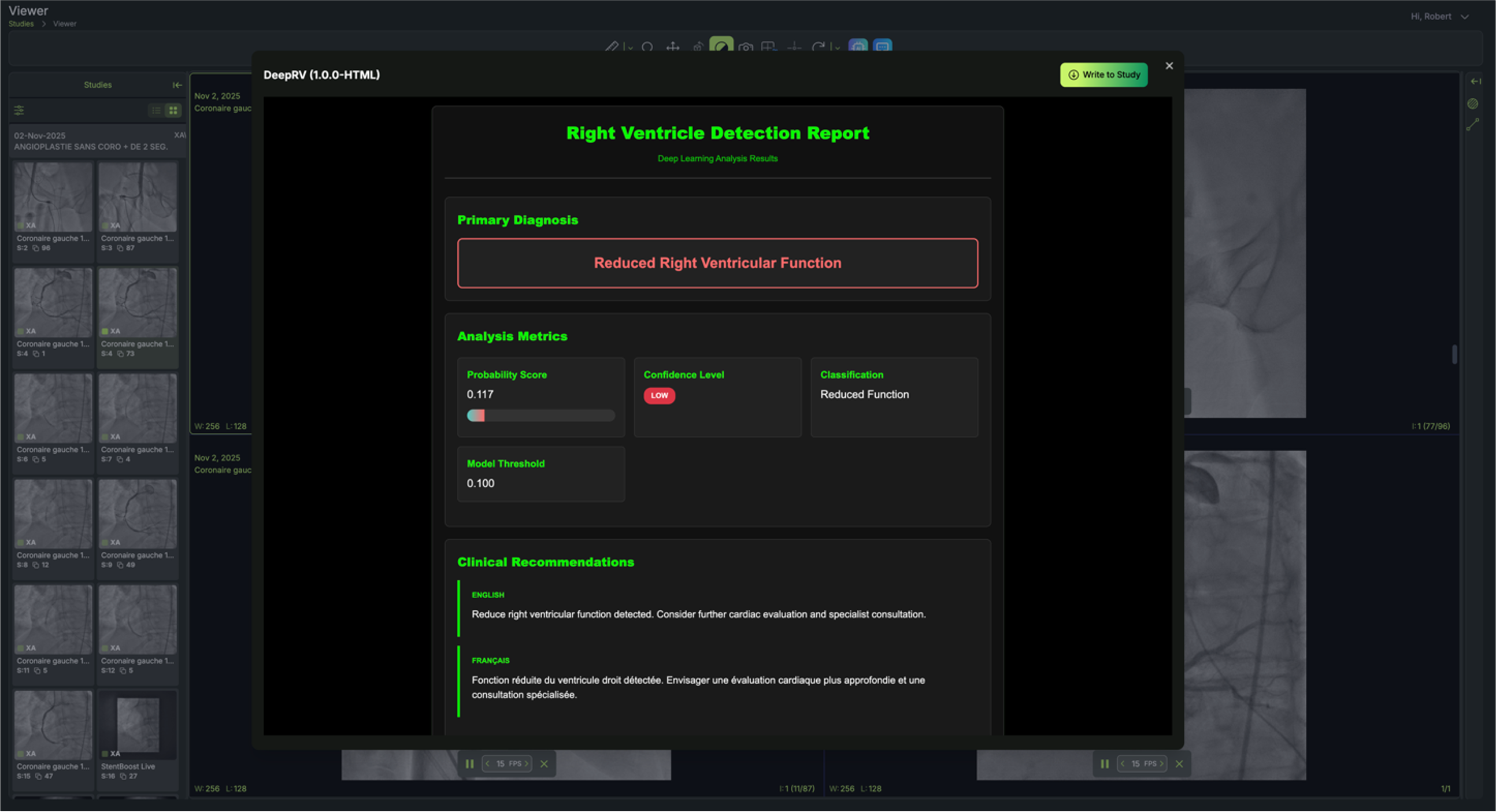
DeepRV runs inside PACS-AI, our DICOM-routing layer that pushes angiograms to AI models the moment they are acquired. The interventionalist sees the RVSF prediction at the point of care, before leaving the lab.

To confirm DeepRV captures RV-specific signal rather than simply tracking LV function, we compared it to CathEF, our previously published angiogram-based LVEF model. In patients with reduced LVEF (<40%), DeepRV significantly outperformed CathEF (AUROC 0.759 vs. 0.661, p=0.006). A combined CathEF+DeepRV model achieved the highest overall discrimination (AUROC 0.833).
A 69-year-old woman presented with cardiac arrest and inferior STEMI on initial ECG which subsequently normalised. Despite an angiographically patent RCA and resolved ST-elevation, DeepRV flagged reduced RV function. Six hours later she deteriorated, requiring vasopressors; TTE confirmed acute RV failure. After RCA stenting, the DeepRV score normalised — illustrating real-time detection of reversible RV dysfunction beyond standard angiographic assessment.
Funded by Fonds de recherche du Québec (FRQ 5232) and an FRQS career award to Dr. Robert Avram.